About Infantile Hemangioma
Infantile hemangiomas are benign vascular tumors characterized by the proliferation of the endothelial cells.1 These lesions are rarely present at birth, but appear within the first few weeks of a child’s life.2
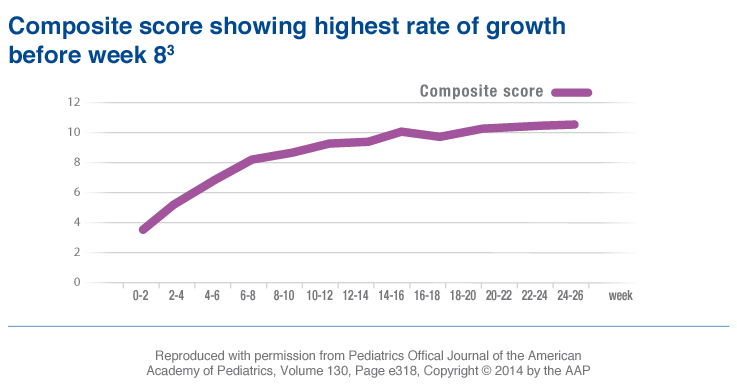
The evolution phases of infantile hemangioma growth include3-5:
- The proliferation phase: rapid growth between 5 ½ and 7 ½ weeks of age that can last up to 6 months or longer3,4
- The involution phase: stabilization then a slow, spontaneous regression over a span of 3 to 9 years5
The Cause of Infantile Hemangioma
It is not well understood what causes infantile hemangiomas. However, studies indicate that fetal hypoxic stress might trigger proliferation and abnormal blood vessel formation by stimulating endothelial progenitor cells.
Another hypothesis is that immature endothelial cells and pericytes, which coexist in the late stages of fetal development, may maintain persistent proliferation properties for a period of time after birth, leading to the development of infantile hemangioma.2
Population at risk
Low birth weight
Female
Caucasian
Multiple gestation
Premature infants
Diagnosis and Treatment
Diagnosis of infantile hemangioma requires a physical examination along with review of the patient’s medical history, including determining how long the infantile hemangioma has been present and if it has changed.
Although infantile hemangiomas are often diagnosed based on a physical examination and medical history, in some cases, imaging tests can also be helpful.7
Magnetic resonance imaging (MRI) can help differentiate infantile hemangiomas from other vascular lesions, such as arteriovenous or venous malformations. A skin biopsy can also be helpful in distinguishing unusual or atypical hemangiomas from other vascular lesions.8 GLUT-1 is an exclusive marker for infantile hemangioma and is used to distinguish infantile hemangiomas from other vascular lesions. Using glucose transporter 1 (GLUT-1) stain is helpful in evaluating tissue removed during a biopsy or excision. Proliferating and involuting infantile hemangiomas stain positively for GLUT-1, while other cutaneous vascular neoplasms, malformations, and normal cutaneous vasculature do not, making this stain very sensitive and specific for histologic confirmation of infantile hemangiomas.9
It may be important to refer to a specialist, such as a pediatric dermatologist, to help confirm a diagnosis and find the most appropriate treatment for your patient as soon as possible.2 Early treatment during the proliferation phase between 1 month to 5 months is important.3
Early Therapeutic Intervention During the Proliferation Phase of Hemangioma Growth Is Essential
Types of Infantile Hemangiomas
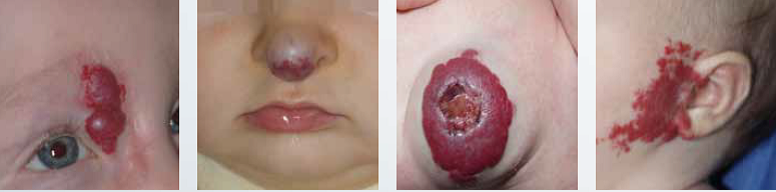
Infantile hemangiomas can be divided into superficial hemangiomas, subcutaneous (deep) hemangiomas, and mixed hemangiomas. All types of infantile hemangiomas are slightly warm to the touch.1
- Superficial hemangiomas are often described as “strawberry marks” and appear as a bright red tumor with an irregular surface Account for 50% to 60% of all infantile hemangiomas
- Subcutaneous or deep hemangiomas present as protruding tumors appearing under normal or bluish skin Make up approximately 15% of all infantile hemangiomas
- Mixed or combined hemangiomas exhibit a combination of both superficial and subcutaneous characteristics Account for 25% to 35% of infantile hemangiomas

From left to right: 1. Superficial hemangioma; 2. Mixed hemangioma; 3. Mixed and ulcerated hemangioma;
4. Superficial hemangioma; 5. Nodular hemangioma;
Morphological Subtypes of Infantile Hemangiomas
Focal (localized) 1
- Located on the bony prominences
- 60% are located on the head and neck
Multifocal 2
- Multiple hemangiomas that can range in number
Segmental 3
- Cover 1 or more segments of the face and body
- Can grow for up to 2 years
Most infantile hemangiomas are the nodular type, which are discrete, oval or round, and usually not associated with malformations. However, segmental hemangiomas are at a higher risk for complications like frequent ulceration. Segmental hemangiomas may have visceral involvement of internal organs, including the liver, gastrointestinal tract, cardiovascular system and brain.1
Segmental hemangiomas may also be associated with developmental abnormalities, including PHACE syndrome, PELVIS syndrome (also known as SACRAL syndrome).1
The acronym for PHACE stands for4:
- Posterior fossa anomalies
- Hemangioma
- Arterial lesions
- Cardiac and aortic abnormalities
- Eye abnormalities
About 20% of segmental infantile hemangioma are associated with PHACE syndrome—88% of which are females.1
- Perineal hemangiomas
- External genital malformations
- Lipomyelomeningocele
- Vesico-renal anomalies
- Imperforate anus
- Skin tag

1. Léauté-Labrèze C,Prey S, Ezzedine K. Infantile haemangioma: part I. Pathophysiology, epidemiology, clinical features, life cycle and associated structural abnormalities. J Eur Acad Dermatol Venereol .2011;1-9. [epub ahead of print]
2. Hemangioma Investigator Group website. Multiple hemangiomas. https://hemangiomaeducation.org/info_multiple.html. Accessed February 28, 2014.
3. Vascular Birthmark Institute website. Hemangiomas – Segmental. https://www.vbiny.org/photo-gallery/hemangiomas/segmental. Accessed February 10, 2014.
4. Tollefson MM, Frieden IJ. Early growth of infantile hemangiomas: what parents’ photographs tell us. Pediatrics. 2012;130(2):e314-e320.
5. Girard C, Bigorre M, Guillot B, Bessis D. PELVIS syndrome. Arch Dermatol. 2006;142:884-888.
7. American Academy of Orthopaedic Surgeons website. Hemangioma.
8. Antaya RJ. Infantile hemangioma. 2007:1-20.
9. Lowe LH, Marchant TC, Rivard DC, Scherbel AJ. Vascular malformations: classification and terminology the radiologist needs to know.
The Classification of Vascular Anomalies
There are 2 classifications of vascular anomalies, including vascular tumors and vascular malformations.
The most common type of vascular tumor is infantile hemangioma.
Other types of vascular tumors include 1
- Congenital hemangioma
- Tufted angioma
- Kaposiform hemangioendothelioma
- Spindle cell hemangioendotheliomas
- Epithelioid hemangioma
- Hemangioendotheliomas
- Others
Types of vascular malformations include1
Simple:
- Capillary malformation (CM)
- Venous malformation (VM)
- Lymphatic malformation (LM)
- Arteriovenous malformations
- Arteriovenous fistula
Combined vascular formations:
- Capillary venous malformation (CVM)
- Capillary lymphatic malformation (CLM)
- Capillary-arteriovenous malformation (CAVM)
- Lymphatic-venous malformation (LVM)
- Capillary-lymphatic-venous malformation (CLVM)
- Capillary-lymphatic-arteriovenous malformation (CLAVM)
- Capillary-venous-arteriovenous malformation (CVAVM)
- Capillary-lymphatic-venous-arteriovenous malformation (CLVAVM)
Anamalies of major named vessels
Anomalies of:
- Origin
- Course
- Number
- Length
- Diameter
- Communication (AVF)
- Persistence (of embryonal vessels)
Associated with other anomalies:
- Klippel-Trenaunay sydrome
- Parkes Weber sydrome
- Servelle-Martorell sydrome
- Sturge-Weber sydrome
- Limb CM+ congenital non-progressive limb hypertrophy
- Maffucci sydrome
- Macrocephaly
- CLOVES sydrome
- Proteus sydrome
- Banayan-Riley-Ruvalcaba sydrome
Vascular tumors grow mainly by endothelial cell hyperplasia whereas vascular malformations have a quiescent endothelium (inner lining) and are considered localized defects of vascular morphogenesis.2
While vascular tumors can regress or persist depending on their type, vascular malformations persist throughout a child’s life and never regress. Most vascular malformations have commensurate growth during childhood, and some worsen over time if left untreated.2
For help in differentiating vascular tumors from vascular malformations, you can refer to a specialist. A pediatric dermatologist can help determine a proper diagnosis and find the treatment that is right for your patient.
HEMANGEOL is indicated for the treatment of proliferating infantile hemangioma requiring systemic therapy.
1. ISSVA classification for vascular anomalies. https://www.issva.org/content.aspx?page_id=22&club_id=298433&module_id=152904. Accessed June 9, 2014.
2. Enjolras O, Wassef M, Chapot R. Introduction: ISSVA classification. Cambridge University Press website. Accessed February 28, 2014.
The Serious Impact of Infantile Hemangiomas on Patients and Their Caregivers
Infantile hemangiomas are the most common benign tumors of infancy—affecting up to 10% of all infants and up to 30% of premature babies.1 Among these infants, about 12% have complications that lead to ulceration, impaired vision, or disfigurement.2
- Serious complications of infantile hemangiomas include1,3:
- Permanent harm to a child’s vision
- Auditory canal obstruction
- Painful ulceration
For every 10 cm2 increase in the size of a hemangioma, there is an approximately 5% increase in complications.3
- 1/3 of facial infantile hemangiomas will result in soft tissue distortion or damage3
- 69% of infantile hemangiomas leave residual lesions when left untreated4
Infantile hemangiomas may also cause long-lasting psychological effects on parents and caregivers and later on the affected children.
1. Storch CH, Hoeger PH. Propranolol for infantile haemangiomas: insights into the molecular mechanisms of action. Br J Dermatol. 2010;163:269–274.
2. Drolet BA, Frommelt PC, Chamlin SL, et al. Initiation and use of propranolol for infantile hemangioma: report of a consensus conference. Pediatrics. 2013;131(1):128-140.
3. Haggstrom AN, Drolet BA, Baselga E, et al. Prospective study of infantile hemangiomas:clinical characteristics predicting complications and treatment. Pediatrics. 2006;118(3):882-888.
4. Bauland CG, LÜning TH, Smit JM, Zeebregts CJ, Spauwen PHM. Untreated hemangiomas: growth pattern and residual lesions. Plast Reconstr Surg. 2011:127(4):1643-1648.
5. Tollefson MM, Frieden IJ. Early growth of infantile hemangiomas: what parents’ photographs tell us. Pediatrics. 2012;130(2):e314-e320.